As a physician who has followed the issue of “end of life” pathways closely over the last 15 years, the contents of the report “When End-of-Life Care Goes Wrong” (WELCGW) – published on March 2 by the UK Lords and Commons Family and Child Protection Group – are not a surprise. However, they are tangible proof that end-of-life pathways have infiltrated back into the health system and are widespread throughout the NHS, and are tainting the good name of palliative care.
Six hundred families have come together as a clear statement that these end-of-life pathways are assailing families and leaving them bereaved and without closure. How did this situation come about?
Dame Cicely Saunders was the doyenne of the modern hospice movement that she started over 50 years ago. She recognised that patients who were dying needed compassion and respect and that they should not be abandoned by their doctors but continue to receive the best medical care. She said that “many patients feel deserted by their doctors at the end”, but the doctors needed “to keep the patient’s own struggle within his compass and to bring hope and consolation to the end”. She was strongly against euthanasia and said that true palliative care “regards dying as a normal process and never hastens nor postpones death”.
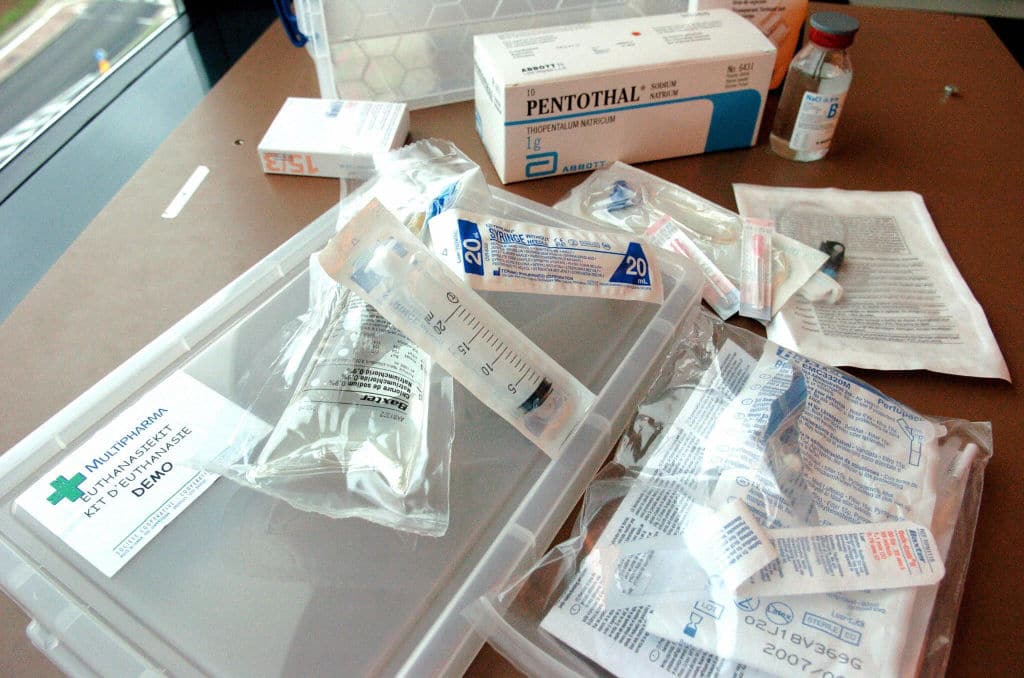
The first clear departure from her principles was the Liverpool Care Pathway (LCP). The key component of the LCP was a mechanical syringe that contin-uously delivered three medicat-ions, of morphine (a painkiller), midazolam (a sedative) and glycopyrrolate (which reduces saliva). A nurse gradually increased the doses without the need for a doctor’s input, but based on a patient’s symptoms.
The LCP was successfully used on dying cancer patients, so was extended to all patients who were deemed to be “dying”. It was quickly taken up into the NHS after 2005 and by 2012, 29 per cent of all NHS patients were dying on the LCP. An increasing public outcry against inapprop-riate deaths from the pathway caused the government to set up an enquiry (the Neuberger Report) which discontinued the use of the LCP in 2013.
Although it departed so far from the principles set out by Dame Cicely, the LCP had continued to be called “palliative care” and palliative-care teams delivered it. The LCP stopped, but palliative-care practitioners spread and continue to work in the NHS. However, with the WELCGW we find that there is much in the end-of-life pathways that is identical to the LCP.
Palliative care is now included by the World Health Organisation as a human right of health. The WHO says: “Palliative care improves the quality of life of patients and that of their families who are facing challenges associated with life-threatening illness, whether physical, psychological, social or spiritual. The quality of life of caregivers improves as well.” The WELCGW report reveals that there are at least 600 famil-ies for whom this is not true.
A year ago, it was announced that “dying people will be given an explicit legal right to healthcare for the first time in NHS history, requiring every part of England to provide specialist palliative care”. So palliative care is becoming a legal right if you are “dying”.
The problem is that it is impossible to diagnose with any reasonable certainty that someone actually is dying. Even a very experienced clinician cannot do this. Who then is this “right” going to be applied to? And how can we be sure that what happened to the patients in the WELCGW report will not keep happening to others?
The latest development of this “right” in Europe is that palliative care is now deemed good for all chronic disease. A new EU initiative to be trialled in Malta states: “Palliative care improves the quality of life of patients with chronic debilitating illnesses or conditions as well as their families’ experiences. Our target is to address palliative needs as early as possible in one’s chronic illness journey.”
So now it is not only the “dy-ing”, but all with chronic disabil-ity. This takes in a large proport-ion of the elderly population. How is it that we have just found out how wonderful palliative care is? How were we coping without it before? The Neuberger Report that discontinued the LCP in 2013 determined that care at end of life should be a continuation of “normal good care due to a patient”.
Pre-set plans like end-of-life pathways tend to take the attent-ion of doctors and nurses off specifically managing the pat-ient’s day-to-day symptoms and treating them. It was found that patients on the LCP died, on average, 29 hours after starting the pathway. Since the same medications are now being used in end-of-life pathways, is there any reason to believe this has changed?
After the WELCGW report end-of-life pathways can no longer be trusted to “care” and not to bring about death. It may sound reassuring to some to say that palliative care improves quality of life and ensures human dignity at all stages of an illness. However, the LCP was said to “drive up the quality of dying”. Who can objectively assess vari-ables like quality of life, dignity and what makes a good death?
St John Vianney tells us that life is given to us so that we may learn to die well. The last days of our lives are the most important – the good thief’s action, at the last hour, took him to heaven. Our last few days are spiritually crucial to put ourselves at rights with the Lord. The worst of end-of-life pathways is not only that they hasten death but that they may prevent us from repenting for sins undeclared, and from dying well and reaching our heavenly goal.
Those who judge a “good death” by the external appearance of serenity are all too ready to use opiates and midazolam to reach this. In so doing they may take away our last chance of confession and forgiveness. For Catholics this is the most sinister trap of end-of-life “care”.
One major nagging concern about the widespread enthusiasm for palliative care is about finances. Where is the money for all these new palliative-care teams coming from? One of the factors that greatly facilitated the LCP was that it saved NHS trusts expenditure, since the sick elderly tend to have long and expensive stays in hospital.
A recent missive from WHO/Europe about the need for more palliative care, published on openaccessgovernment.org, states: “One way to manage this rise in costs is to ensure a better balance between disease treatment and the management of symptoms at the end of life.” How does “management of symptoms” differ from disease treatment? And how does one ensure a “better” balance? Is this simply a euphemism for euthanasia?
The Revd Dr Patrick Pullicino is a retired NHS consultant neurologist and assistant priest at St Bede’s, Clapham Park, in the Archdiocese of Southwark
Areas of Catholic Herald business are still recovering post-pandemic.
However, we are reaching out to the Catholic community and readership, that has been so loyal to the Catholic Herald. Please join us on our 135 year mission by supporting us.
We are raising £250,000 to safeguard the Herald as a world-leading voice in Catholic journalism and teaching.
We have been a bold and influential voice in the church since 1888, standing up for traditional Catholic culture and values. Please consider donating.